Menstruation usually begins around 11 years of age, but there is a wide variation in this and anytime between 9-14 years is normal. If onset of menses is delayed beyond this, examination and tests of the girl are required to confirm that there is no problem.
Initially, the periods can be very irregular and may not become regular upto 12 – 18 months of starting. This is due to immaturity of the hormone axis and is normal. Too heavy bleeding during menses needs check up and treatment as it may be a sign of a bleeding disorder or hormonal problem and can result in anemia and weakness. Gradually the menses will normalize and the girl will bleed for 3 – 5 days every 28-30 days, which is the normal cycle.
Menstrual hygiene is very important and must be taught to all young girls. Frequent baths during the periods, changing pads frequently, disposing off the pads hygienically is absolutely necessary. Even today, there are lots of myths about menstruation like not eating pickle, not entering the kitchen, taking total rest during this time etc., all of which are illogical.
The adolescent girl is going through a lot of hormonal changes in her body which reflect in her physical, mental and emotional state. Mood changes, irritability, emotional swings are related as much to hormones as to environment. The attitude of the family towards menstruation will help her deal with it for the rest of her life. If it is treated as dirty, unclean and she is isolated, she will have a negative response to menses forever. If it is treated as a wonderful process of growing up or maturing and having the amazing ability to bear children later, she will treat it positively and it has been shown that these girls get much lesser pain and discomfort during menses as well as less premenstrual syndrome (PMS)
During the teenage years many girls experience PMS. This may cause bloating, breast pain, depression and irritability prior to menses and the symptoms disappear after the periods. This is perfectly normal and restriction of salt, refined flour, caffeine and chocolates alongwith light exercise during this time helps relieve symptoms. Also addition of calcium, B-complex, primrose oil and such supplements may help reduce symptoms. Occasionally, hormone treatment is required in severe cases.
Painful periods (dysmennorhoea) is another common problem in teenagers and many girls miss school and college because of it. This is usually due to excessive local production of prostaglandin’s and can be reduced by light exercise, hot showers and antiprostaglandin tablets taken at the onset of menses. In some girls regular hormonal pills have to be given if there is severe pain.
Often during the growing years, there is a variation in the size of both breasts and this causes immense worry to the girl. This variation is common, may sort itself out once full growth is achieved or once in a while the discrepancy may remain till adulthood. This has to be managed by wearing a suitability-padded bra or later by surgery and there are no creams or medicines, which can help this.
There are many myths associated with menstruation and growing up and proper sex education and counseling or a meeting with a good gynaecologist should be a part of growing up.
{kind=link}
{kind=link}
{kind=link}
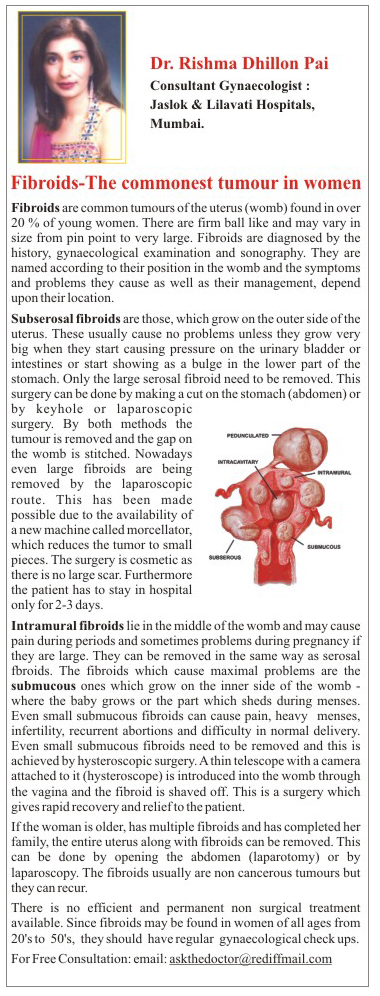
Fibroids are common tumours of the uterus (womb) found in over 20 % of young women. There are firm ball like and may vary in size from pin point to very large. Fibroids are diagnosed by the history, gynaecological examination and sonography.
They are named according to their position in the womb and the symptoms and problems they cause as well as their management, depend upon their location.
Subserosal fibroids are those, which grow on the outer side of the uterus. These usually cause no problems unless they grow very big when they start causing pressure on the urinary bladder or intestines or start showing as a bulge in the lower part of the stomach. Only the large serosal fibroid need to be removed or those, which are of the stalk, need to be removed as they can get twisted. This surgery can be done by making a cut on the stomach (abdomen) or by keyhole or buttonhole (laparoscopic) surgery. By both methods the tumour is removed and the gap on the womb is stitched. Nowadays even large fibroids are being removed by the laparoscopic route This has been made possible due to the availability of a new machine called morcellator,which reduces the tumor to small pieces. The surgery is cosmetic as there is no large scar . Furthermore the patient can go home in a couple of days.
Intramural fibroids lie in the middle of the womb and may cause pain during periods and sometimes problems during pregnancy if they are large such as preventing a normal delivery, heavy bleeding or infection after delivery. They can be removed in the same way as serosal fibroids.
The fibroids which cause maximal problems are the submucous ones which grow on the inner side of the womb - where the baby grows or the part which sheds during menses. Even small submucous fibroids can cause pain, heavy and irregular menses, infertility, recurrent abortions and difficulty in normal delivery. Even small submucous fibroids need to be removed and this is achieved by hysteroscopic surgery. A thin telescope with a camera attached to it (hysteroscope) is introduced into the womb through the vagina and the fibroid is shaved off. This is a surgery which gives rapid recovery and relief to the patient.
If the women is older, has multiple fibroids and has completed her family, the entire uterus along with fibroids can be removed. This can be done by opening the abdomen (laparotomy) or by laparoscopy.
The fibroids usually are non cancerous tumours but they can recur. Hence even if all fibroids are removed - new ones may grow in a couple of years.
There is no efficient and permanent non surgical treatment available and once a month injections can only temporarily shrink the fibroids.
Nowadays, the fibroid can be treated by passing a catheter through an artery in the thigh right upto the womb and blocking the blood supply of the womb by injecting small sponge like material under X-ray control. This is called uterine artery embolization and is being practiced in a few places though it is still not the most accepted method of treatment.
Since fibroids may be found in women of all ages from those in 20’s to those in their 50’s, it is best to have a gynaecological check up if there are any symptoms.
{kind=link}
Q.1. I am 28 yrs. old and suffer from pain during my periods. I was diagnosed as having a large fibroid when I did a sonography recently. Are there any medicines that will treat this fibroid or do I have to undergo surgery? Reena
Ans: Fibroids are non-cancerous tumours which if large and placed deep inside the uterus (womb) can cause heavy menstrual bleeding, pain, infertility and abortions. There is no permanent cure with medicines and removal of fibroids is the only option in a young woman like you. This can be done by Keyhole surgery (laparoscopy) in which even large fibroids can be removed through a 1-2 cm cut on the stomach (abdominal wall). If the fibroid is on the inner side of the womb, it can be shaved off with the help of a hysteroscope and this can be done without any cuts or stitches. The recovery from these surgeries is very good and hospitalization is for 1-2 days only. Some cases may require an open surgery with a 3-4 inch cut on the abdomen.
Endometriosis is a common problem which affects young women in the reproductive age group. In this, the tissue which lines the womb (endometrium) is found growing in abnormal locations such as the ovaries or around the uterus.
Every time the patient has her menses, there is also bleeding inside this. As a result thick dark blood accumulates in the ovaries (endometrium cyst) and there are blood spots all over the pelvis which cause the intestines tubes and ovaries to stick to each other.
Endometriosis can cause severe pain before or during periods, also heavy or abnormal bleeding. As it damages tubes and ovaries, it often causes infertility (inability to conceive). The condition always worsens with time and in severe cases can result in total damage to all pelvic organs causing a frozen pelvis.
The diagnosis is made by history, examination and sonography. Sometimes a laparoscopy (Key hole surgery) may be required to diagnose and treat endometriosis at the same time.
The treatment is essentially surgical. Nowadays, 2-3 visual cuts on the stomach wall are used to introduce a camera and operating instruments inside the pelvis and the endometriotic areas are removed and burnt using current or laser.
Despite surgical removal, there is a possibility of recurrence of endometriosis, and the same patient needs multiple surgeries within a few years.
Medical treatment is used to create ‘artificial menopause’ as when there are no periods, the endometriosis subsides. This can be done using continuous hormone tablets or once a month injections. However this form of treatment is temporary.
Young patients with endometriosis who want to have a baby may require specialized treatment like IUI or IVF (Test tube baby). If the patient is older and has had repeated surgery, a total hysterectomy with oophoorectomy (removing uterus and ovary) is the final solution.
{kind=link}
{kind=link}
Adenomyosis is defined as the presence of endometrial glands and supporting tissues in the muscle of the uterus where it normally would not occur. When that gland tissue undergoes growth during the menstrual cycle and then subsequent sloughing, the old tissue and blood cannot get out of the muscle and flow out of the cervix as part of normal menses. This trapping of the blood and tissue causes uterine pain in the form of menstrual cramps. It also produces abnormal uterine bleeding as some of the blood finally escapes the muscle and results in prolonged spotting.
Adenomyosis occurs more often in the decade of the 40's, perimenopausally. In hysterectomy specimens, adenomyosis can be found from 15% to 25% of the time (1, 2). The glandular change of the endometrial cells in adenomyosis are often incomplete in the second half of the menstrual cycle (luteal phase) and as a result, adenomyosis may not be very responsive to suppression by progesterone. About 50% of adenomyosis is asymptomatic although as it goes deeper into the uterine muscle it tends to be more likely to produce symptoms (3, 4). It is also often associated with fibroids (5 and often associated with other conditions such as ovarian cysts, prolapse and even gynecological cancers (6) that can cause pelvic pain.
NEW TECHNIQUES IN THE MANAGEMENT OF ABNORMAL UTERINE BLEEDING:
Excessive uterine bleeding is one of the commonest problems encountered in gynecological practice and accounts for 15-20% of all gynecological admissions in an institution.
When the uterus shows no major pathology, this excessive bleeding is labeled as dysfunctional uterine bleeding (DUB). Traditionally DUB has been managed by prolonged hormonal therapy, repeated D& C’s or hysterectomy. Today, however there are new conservative simple techniques available to effectively and permanently treat DUB.
Transcervical resection of endometrium (TCRE) using the resectoscope was the first such conservative procedure using similar principals to that of TURP done by the urologists. Yet, today TCRE has lost its popularity due to the high incidence of severe complications such as uterine perforation with bleeding and burns, glycine overload and the expertise needed to carry out this procedure.
Uterine balloon ablation (UBT) is a simple, short, safe and permanent procedure to treat DUB. It consists of a catheter, similar to a foley’s catheter, which is connected to a computerized device to control temperature and pressure. This catheter is introduced through the vagina into the uterus and the balloon is inflated with dextrose. The heating device within it is started and temperature is raised to 87 degree centigrade. The balloon pressure is maintained at 160-180 mm of mercury. In 8 minutes the entire endometrium is permanently dessicated. The balloon is deflated and catheter removed.
This procedure can be done under local anaesthesia with sedation or with a short general anaesthesia. It is an OPD procedure. In the past few years I have done this procedure on a large number of patients including those with renal failure, coagulation disorders, gross obesity and multiple previous surgeries in whom a hysterectomy would have been too high risk a procedure. Even in this group there have been no complications.
This procedure is being successfully done in Jaslok Hospital. Mumbai.
- Breast cancer
- Cervical Cancer
- Ovarian cancer
- Vulvar Cancer
- Uterine Cance
FAQ
Q.1. I am 40 years old and I have heard my friends saying that they have done a PAP smear. What is it exactly and does everyone in this age group have to do one? Kavita
Ans: 40 is the age group at which one recommends that every woman should begin regular cancer check ups in order to prevent missing out on early diagnosis of any cancer or tumor. PAP smear is a simple test where a brush or cotton swab is touched to the cervix (the opening of the womb) and a slide is prepared, which is then analyzed to look for any abnormality such as cancer. This is a simple test and can be done in a doctor’s clinic in 2 minutes. This test should be repeated every year and should be started from the time a women is sexually active.Also at 40, you must undergo a pelvic sonography to rule out cancer of the womb or the ovary and a mammography to look for any breast tumour. These tests form the basis of cancer screening in women.
Q.2. I am 53 years old and have been menopausal since 3 years. I have suddenly started having little vaginal bleeding again. Can this be anything serious? Do I need a check up? Priyanka
Ans: Once the periods have stopped for one year then menopause is established. After that you should never have vaginal bleeding again, not even spotting. You need to be immediately checked up by a gynaecologist who will do an internal examination and a PAP smear to rule out cancer of the cervix (mouth of the uterus). You should also undergo a sonography to look for swelling of the uterine lining which may indicate endometrial hyperplasia or cancer or an ovarian tumour, all of which may cause vaginal bleeding.
Vaginal/pelvic organ prolapse occurs when an organ in the pelvis, such as the bladder or uterus, falls or slips out of place, into the vagina. The rectum and intestine can also prolapse into the vagina. Bladder prolapse may also be called a cystocele. Uterine prolapse is also referred to as a pudendal hernia or pelvic floor hernia.
{kind=link}
FAQ
Q.1. I am 38 years old and have had two normal deliveries. Now I feel that something is coming out of my vagina when I strain, as if my uterus has dropped down. Also my husband complains that the vagina feels loose when having intercourse. Are there some exercises to improve this condition? Ruchi
Ans: You probably have a prolapse of the uterus and vaginal laxity which can occur following difficult normal deliveries or operative vaginal delivers such as forceps delivery. The condition will never improve but may worsen after menopause. You can do pelvic floor exercises called Kegels exercises which can help slightly, but the main treatment is surgical. The vagina can be tightened by a simple procedure called ‘Perineal repair’ which is a short and easy procedure, and the vaginal tightness can be restored to the pre-delivery situation. The uterus which has come down, can be pulled up and fixed by either a small bikini cut on the lower part of the stomach or even by Keyhole (laparoscopic surgery). These procedures are safe and give very good results
How can I be sure this is SUI?
A simple gyneclogical examination on a full bladder , by your doctor , can clinch the diagnosis. There are specific tests, such as urodynamic study which can differentiate SUI from irritable bladder or failure of the valve mechanism of the urethra.
Do I need to undergo treatment for this?
SUI is not going to improve on its own, it will probably worsen, especially after menopause. There are conservative treatments such as physiotherapy, pelvic floor exercises (Kegels exercise), electric stimulation etc which may lead to some improvement in symptoms. However these are for mild cases only and results may not be guaranteed.
What are the surgical options for me?
There are many different types of surgeries available and the choice can be made after seeing the nature of the problem and the doctor’s preference. SUI may be accompanied by sagging of the bladder wall or cystocoele. Both these can be tackled by vaginal cystocoele repair along with the traditional kelly’s stitch, which is a vaginal approach.
Are there any newer methods of treatment available?
Nowadays the preferred surgeries are open or laparoscopic Burch colposuspension operation, sling operations or needle procedures. The latest techniques are those of TVT (tension free vaginal tape) where a tape is inserted from the vagina and fixed below the middle of the urethra. This is done under local or spinal anaesthesia.
The newest modification is to pass the tape under the bladder opening and bring it out through the obturator foramen situated on the medial side of the thigh, a shorter and simpler procedure. Most of those procedures give good results and recurrence rates are low.
How risky are these surgeries?
All surgeries come with a certain amount of risk . But most of the surgeries are quick and require no prolonged hospitalization.
Dos & Donts
- Make sure your deliveries are conducted under supervision.
- Pelvic floor exercises are to be done lifelong.
- You don’t have to live with the embarassment of SUI.
- Alternate forms of treatment can be tried.
- Simple & short surgical options are available.
FAQ
Q.1. I am 36 years old with two normal deliveries. Since one year, every time I cough or sneeze, I pass urine in my underclothes. This is very embarrassing. As a result I have stopped going out and I wear a pad at all times. What do I do? Samiksha
Ans. This is known as Stress urinary incontinence (SUI). Sometimes due to the stretching and loosening of the pelvic floor due to normal deliveries, repetitive strenuous work or inherited tissue weakness there is weakening of the support of the urinary outlet tube (urethra). So whenever there is increased pressure due to coughing / sneezing, the urine leaks out. This may result in a feeling of wetness and a continuous urine smell from the underclothes. Often, it may interfere with your day-to-day social activities. This usually requires surgical treatment and nowadays simple effective treatment such as TVT and TOT are available which require only one day stay in hospital, no cuts or stitches on the stomach and rapid recovery. Some new drugs have come into the market-which can be tried in mild cases.
5 –25 % of all women between 15 – 65 years leak urine involuntarily. This is an extremely embarrassing problem and women are scared to venture out of the house if they are not able to control urine effectively. Some women use pads or diapers in order to hide this problem. This lack of control of urine may be Stress urinary incontinence (SUI), which is leakage of urine when the woman coughs, sneezes or laughs loudly. It may be otherwise be a condition called an unstable bladder which is characterized by an increase in frequency of urination, inability to control it and leakage of urine before reaching the bathroom, and getting up at night to go the bathroom. Many women develop these problems after vaginal delivery due to the stretching and tearing of the vagina during a difficult delivery. After menopause there is a loss of hormones which result in thinning, dryness and weakness of the bladder supports and this can result in inability to control urine.
These have different treatments and so a clear diagnosis must first be made.
A urine check, sonography of the bladder and kidneys and a special test called urodynamic study will help arrive at an accurate diagnosis. Sometimes looking inside the bladder, with a telescope (cystoscopy) may be required. Wrong diagnosis may result in more problems than benefits.
The treatment of Stress incontinence is essentially surgical, though some people may benefit by pelvic floor exercises known as Kegels exercises. Surgical treatments may vary from surgery to pull up the bladder neck which can be done by open surgery or by key hole surgery (laparoscopy). The newer techniques however are easier and faster and give good results. These involve placing a tape just above the urinary opening near the vagina. These are the tension free vaginal tape (TVT) procedure or the Transobturator tape (TOT) procedure. In this there are no visible stitches on the patients abdomen and only one or two stitches near the urinary opening are required. Following these procdures, the patient can go home in one day. Few cases can be treated by injecting special material on both sides of the urinary opening.
The urge incontinence however is better managed with medicines which reduce the bladder irritability and surgery is rarely required. In menopausal women, estrogen creams or tablets may help. In some cases dilatation of the urinary opening may need to be done
‘Prolapse’ or coming down of the womb (uterus) or looseness of the vagina is a common problem particularly in women in women in their 40’s and 50’s, especially in women who have had normal deliveries in the past. However even young women without children can get prolapse if they have an inherent weakness o the tissues which support the womb.
The main symptom is the women feels something coming out of the vagina when she strains or on standing. This may be the womb (uterus) coming down or the urinary bladder (cystocoele) or the area close to the rectum (rectocoele)
Often associated with this are urinary problems such as leaking urine or coughing or sneezing (stress incontinence), difficulty in holding urine for long or incomplete emptying of the bladder. There is a feeling of lower abdominal heaviness and low backache. Prolapse also interferes with sexual satisfaction for both the partners.
The problem of prolapse often begins with normal delivery, especially when there is a big baby, prolonged labour, forceps delivery, and vaginal tears. Chronic medical conditions such as asthma, chronic cough, constipation, diabetes and obesity contribute to prolapse. With the onset of menopause and decline of estrogen, there is weakness of tissues and that is when the prolapse becomes severe.
The treatment of prolapse is mainly surgical. In a young woman the treatment will be conservative so as to not damage the womb or the ability to have children later. This may include only a tightening of the vagina and its supports. This is a simple short procedure done from inside the vagina and there are no stitches outside. If the entire womb has come down, it has to be lifted up with the help of strong stitches or tape. This procedure can be done with the help of a laparoscopic (keyhole) surgery with 2 – 3 small cuts on the lower belly or with the help of a small bikini scar.
In older women who have completed her family, the procedure may involve a hysterectomy (removal of the womb), which is done from the vagina combined with a tightening of the area and repair of the urinary leakage if present. This requires few days of hospitalization. Recovery is usually fast from these procedures.
In very old women who are unfit for surgery and have severe prolapse, a rubber ring can be inserted in the vagina as a temporary measure to replace the womb which is coming out. But if used for long this can cause ulcers in vagina and infections.
Essentially the focus should be on prevention. Maintaining healthy lifestyle exercise, especially kegals pelvic floor exercises, keeping weight under control having properly supervised deliveries and taking care of chronic problems such as cough and constipation will significantly help reduce the incidence of prolapse